

Tennis Elbow: What You Need to Know
Pain on the outside of your elbow when gripping, pouring the kettle, using tools, or doing backhand strokes? This guide explains tennis elbow (lateral epicondylalgia)—what it is, common triggers, when to scan, and what actually helps. It also links to our exercise library and a quick video explainer you can watch on the page.
Exercise Library
To access the exercises you need, click the links below.
Level 1 – Isometric Supination
Level 2 – Isotonic Supination
What is tennis elbow?
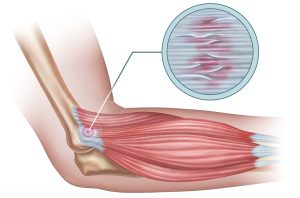
Also called lateral epicondylalgia or historically lateral epicondylitis, tennis elbow is an overload-and-irritation problem of the common extensor tendon, most often the extensor carpi radialis brevis (ECRB) where it attaches to the lateral epicondyle of the humerus. Think of the tendon like a rope: with repetitive gripping and lifting—especially with the knuckles-up (wrist extended) position—it can fray and become sensitive.
It’s not only from tennis. DIY, computer mousing, prying, pouring, screwdrivers, repetitive lifting, or sudden spikes in training/workloads are typical culprits.
Common causes & triggers
-
Spike in gripping/lifting load, especially knuckles-up or with the elbow straight out in front
-
Repetitive wrist extension (backhand, tools, pouring)
-
Reduced forearm and shoulder strength/endurance
-
Poor load distribution (doing everything with one hand, awkward postures)
-
Contributing neck/shoulder stiffness or work-set-up issues
Typical symptoms
-
Localised outer elbow pain; sometimes a line of ache down the forearm
-
Pain gripping, wringing towels, pouring a kettle, opening jars
-
Tenderness over the lateral epicondyle
-
Morning stiffness; worse after repetitive use
-
Reduced pain-free grip strength
Do I need a scan?
Not at the start. Diagnosis is clinical. Consider ultrasound or MRI if:
-
there was a traumatic event with persistent weakness,
-
symptoms persist >12 weeks despite good rehab and load changes, or
-
you’re considering procedures (e.g., injection) or to rule out other causes.
What actually helps (evidence-aligned)
1) Load management (immediate)
-
Change the grip: palms-up where possible; second choice thumbs-up; last choice knuckles-up.
-
Keep the elbow by your side when lifting (reduces tendon compression); avoid straight-arm, out-front lifts.
-
Short “deload” phase if very irritable (3–7 days): reduce painful reps, keep gentle movement.
2) Exercise rehab (the main driver)
-
Isometric holds for pain relief (e.g., wrist extension hold at mid-range, 5×1min, comfortable load).
-
Progress to slow strengthening (concentric/eccentric wrist extension, grip dynamometer or putty, forearm supination/pronation, shoulder/scapular endurance).
-
Add functional progressions (carry variations, task-specific drills) as pain allows.
3) Helpful adjuncts
-
Tendon-offloading taping (counterforce brace) for tasks; remove when not needed.
- Wrist brace (counterforce brace) for tasks; remove when not needed, sounds strange bracing your wrist! But this is the joint the injured muscle/tendon complex supports.
-
Manual therapy/dry needling short term to enable exercise.
-
NSAIDs short course via GP if appropriate.
4) Injections & procedures (if rehab is blocked)
-
Corticosteroid can reduce pain short-term, but relapse is common and outcomes are often inferior to exercise long-term. We don’t use it as first-line.
-
PRP (platelet-rich plasma) is sometimes considered for persistent cases; responses vary—best used alongside a structured loading plan.
-
Surgery is rarely needed; reserved for refractory cases after high-quality rehab.
Self-care tips you can start today
-
Switch everyday tasks to palms-up or thumbs-up grips.
-
Lift with the elbow tucked; avoid long-reach, straight-arm carries.
-
Break up repetitive tasks (tools, keyboards); micro-breaks 30–60 seconds every 20–30 minutes.
-
Use the counterforce taping and/or wrist brace for heavier tasks only.
-
Keep overall fitness up (walking, cycling) while the elbow calms.
When to seek further help
-
Night pain, pain at rest, or no progress after 2–3 weeks of good load changes
-
Marked weakness, spreading numbness/tingling (rule out nerve issues)
-
Work or sport demands you can’t modify without guidance
How we help
At LivFit Physio Mornington (11 Railway Grove) we’ll confirm the diagnosis, map your pain-free grip strength, and build a staged, progressive plan—with exercise videos you can follow at home. We coordinate imaging or GP review when appropriate, and guide decisions about braces or injections if needed.
If you’d like a Telehealth Consultation with our team, book in Online and select Livfit Physio Mornington and then Initial Telehealth Consultation. I you’d like to see a Physio in person at our Mornington Clinic, book in Online at and select Livfit Physio Mornington and select Initial Consultation.
Call: (03) 5976 8447
Clinic: 11 Railway Grove, Mornington VIC 3931